
Why Dental Implants Don’t Integrate
Why Dental Implants Don’t Integrate, a concern for many prospective patients, represents the primary reason for the failure of what is otherwise one of the most successful and reliable procedures in modern dentistry. With success rates consistently exceeding 95%, dental implants are the gold standard for replacing missing teeth. However, a small percentage of cases do encounter complications, with the most critical being the failure to achieve osseointegration. This biological process, where the implant fuses directly with the jawbone, is the very foundation of a stable and long-lasting tooth replacement. When this fusion doesn’t happen, the implant cannot provide the necessary support for a crown and is considered a failure. Understanding the complex interplay of factors that can disrupt this delicate process is crucial for both patients and clinicians to maximize the chances of a successful outcome.

The Science of Osseointegration: A Foundation for Success
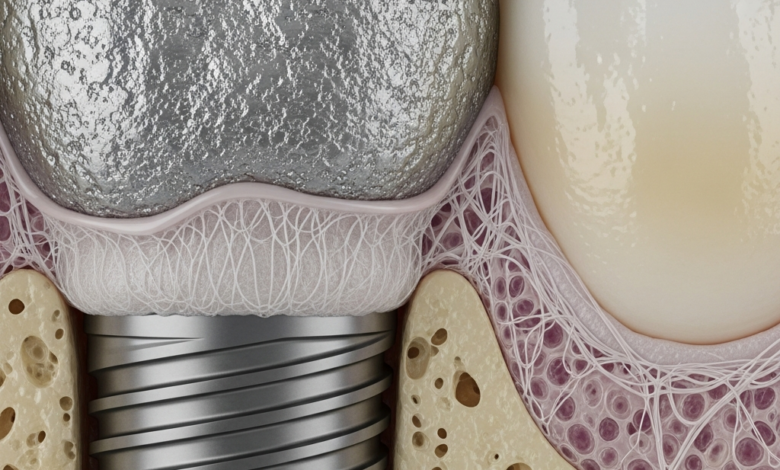
To understand why an implant might fail, one must first appreciate the remarkable biological process that makes it succeed: osseointegration. The term, derived from the Greek *osteon* (bone) and the Latin *integrare* (to make whole), describes the direct structural and functional connection between living bone and the surface of a load-bearing artificial implant. This phenomenon was famously discovered by Swedish orthopedic surgeon Per-Ingvar Brånemark in the 1950s when he observed that titanium chambers he had placed in rabbit femurs had become completely fused to the bone and could not be removed. This discovery revolutionized not only dentistry but also orthopedics.
The process of osseointegration unfolds in several stages:
- Hemostasis and Inflammation: Immediately after the titanium implant is placed into the jaw, blood fills the space between the implant and the bone. This blood forms a clot, which creates a provisional matrix rich in growth factors. This initiates an inflammatory response, bringing healing cells to the site.
- Proliferation and Angiogenesis: In the following days and weeks, new blood vessels begin to form, a process called angiogenesis. This is vital for supplying the area with oxygen and nutrients. Mesenchymal stem cells are recruited to the site and begin to differentiate into osteoblasts, the cells responsible for creating new bone.
- Bone Formation: The osteoblasts start depositing a layer of unmineralized bone matrix, called osteoid, directly onto the implant’s specially treated surface. This is a critical phase where the implant’s biocompatibility and surface texture play a significant role.
- Bone Remodeling: Over several months, this newly formed woven bone is gradually remodeled into stronger, more organized lamellar bone. This mature bone structure provides the immense strength required to withstand the forces of chewing. The entire process requires the implant to remain perfectly still, a concept known as primary stability.
Any disruption to this intricate biological cascade can lead to the failure of osseointegration. Instead of bone, the body may form a soft, fibrous tissue capsule around the implant, which cannot provide any meaningful support.
Early vs. Late Implant Failure: Understanding the Timeline
Implant failure is not a single event; it is typically categorized based on when it occurs. Differentiating between early and late failure helps pinpoint the most likely cause and guides future treatment. Early failure is a direct result of the implant not integrating with the bone, while late failure occurs after successful integration has already been achieved.
| Failure Type | Timing | Primary Causes |
|---|---|---|
| Early Failure | Within the first 3-4 months after surgery (before the final crown is placed). | Lack of primary stability, surgical trauma (bone overheating), contamination, poor bone quality, systemic health issues (e.g., uncontrolled diabetes), smoking. |
| Late Failure | Months or years after the implant has been loaded with a crown. | Peri-implantitis (bacterial infection similar to gum disease), excessive biting forces (bruxism), mechanical failure of components, poor oral hygiene. |
Why Dental Implants Don’t Integrate: The Primary Culprits
The failure of osseointegration is rarely due to a single issue but rather a combination of factors related to the patient’s health, the surgical procedure, and post-operative care.
Patient-Related Factors
The patient’s overall health and habits are paramount to the success of the healing process.
- Insufficient Bone Quality or Quantity: An implant needs a solid foundation. If the jawbone is too thin, short, or soft (low density), it cannot provide the initial mechanical stability required for osseointegration. This is often addressed with bone grafting procedures prior to implant placement.
- Systemic Health Conditions: Certain medical conditions can severely impair the body’s healing capacity. Uncontrolled diabetes, for example, compromises circulation and immune function, increasing the risk of infection and poor healing. Autoimmune diseases and conditions requiring long-term steroid use can also interfere with bone metabolism.
- Smoking: This is one of the most significant risk factors. Nicotine is a vasoconstrictor, meaning it narrows blood vessels, reducing the flow of oxygen and essential nutrients to the surgical site. This can starve the developing bone cells and dramatically increase the failure rate.
- Poor Oral Hygiene: The mouth is home to billions of bacteria. If a patient has poor oral hygiene or pre-existing gum disease, the risk of a bacterial infection developing around the implant (peri-implantitis) is much higher, which can halt osseointegration in its tracks.
Surgical and Procedural Factors
The skill and technique of the surgeon are critical variables in the equation.
- Surgical Trauma: Bone is a living tissue that is sensitive to heat. If the surgeon’s drill overheats the bone during the creation of the implant site, it can cause the bone cells to die, a condition called osteonecrosis. This prevents the bone from ever growing onto the implant surface.
- Lack of Primary Stability: As mentioned, the implant must be completely immobile after placement. If the implant has even microscopic levels of movement, the body will form soft fibrous tissue around it instead of hard bone. The surgeon must achieve excellent initial stability for the process to succeed. For an in-depth review of this topic, a study published in the National Journal of Maxillofacial Surgery provides a comprehensive overview of the causes of implant failure.
- Contamination: The sterility of the surgical environment and the implant itself is non-negotiable. Any bacterial contamination on the implant surface or within the surgical site can lead to infection and subsequent failure.
Recognizing the Problem and Seeking Solutions
Fortunately, when an implant fails to integrate, the signs are usually clear. Early detection allows for prompt intervention and improves the chances of a successful second attempt.
Symptoms of a Failing Implant
While some minor discomfort is normal after surgery, persistent or worsening symptoms are a red flag. The most definitive of all signs of a failed dental implant is mobility; a successfully integrating implant should feel completely solid, just like a natural tooth. Other warning signs include persistent pain or throbbing, swelling of the gums around the implant, or visible threads of the implant.

What to Do If an Implant Fails to Integrate
If you suspect a problem, the first and only step is to contact your dental surgeon immediately. They will perform a clinical examination and take X-rays to assess the bone around the implant. If failure is confirmed, the implant will need to be removed. This is often a simple procedure. The surgeon will then clean the site thoroughly to remove any inflammatory tissue. In many cases, the area may be bone grafted to prepare it for a future implant. After a healing period of several months, a new implant can often be placed with a high probability of success, provided the initial cause of failure has been identified and addressed.





